


棘白菌素的药物敏感性变迁与药敏检测方法的临床应用

王培昌,教授,博士研究生导师。现任首都医科大学宣武医院检验科主任,兼任中华医学会检验分会常委兼临床化学组组长、北京医学会检验医学分会候任主任委员等。近年来共主持国家自然科学基金重点项目1项、国家自然科学基金面上项目4项以及北京市自然科学基金等15项基金资助课题,主编、主译著作5部,以第一作者或通讯作者发表论文200余篇,其中SCI论文45余篇,获北京市科学技术进步奖一等奖1次。

李颖,博士,首都医科大学宣武医院检验科主管技师,从事病原性丝状真菌菌种鉴定、药物敏感性及耐药机制研究工作。以第一作者(或共同第一作者)发表SCI论著6篇,中文核心期刊9篇。
文丨李颖 王培昌
【摘要】近年来,侵袭性真菌感染的临床发病率逐年升高。棘白菌素作为新一代抗真菌药物,因其不良反应少、患者耐受性好、抗菌谱广泛覆盖念珠菌和曲霉两大临床常见病原性真菌而得到较多关注。随着棘白菌素类抗真菌药物在临床的广泛应用,棘白菌素对念珠菌和曲霉的体外敏感性及耐药率发生了改变,相应的棘白菌素体外药敏检测技术也有了更多样的手段,本文就近些年棘白菌素的药物敏感性变迁及药敏检测方法进展进行综述。
【关键词】棘白菌素;药物敏感性;药敏试验
近年来,随着自身免疫病、艾滋病、血液病、肿瘤等疾病的临床发病率不断攀升以及器官移植术等治疗手段在临床的大规模开展,免疫受损病患在临床患者中的比例不断扩大;相应地,侵袭性真菌病(invasive fungal diseases,IFDs)的临床发病率也在逐年升高[1, 2]。目前可用于治疗IFDs的药物主要包括三类,多烯类(代表药物两性霉素B)、唑类(包括氟康唑、伊曲康唑、伏立康唑、泊沙康唑和艾沙康唑)以及棘白菌素类(卡泊芬净、米卡芬净和阿尼芬净)。棘白菌素类抗真菌药物通过非竞争性抑制1, 3-β-D葡聚糖合成酶,干扰真菌细胞壁1, 3-β-D葡聚糖的生物合成,导致真菌细胞壁渗透性改变,细胞溶解死亡。因该类药物引起的不良反应少、患者耐受性好、抗菌谱广泛覆盖念珠菌和曲霉两大临床常见病原性真菌而得到越来越多的关注[3, 4]。随着棘白菌素类抗真菌药物在临床使用程度的不断扩大,以及多重耐药真菌的出现,棘白菌素对念珠菌及曲霉临床分离株的体外药物敏感性及耐药率发生了变迁[5]。棘白菌素药敏检测方法也从经典的微量肉汤稀释法逐步向借助基因检测及MALDI-TOF MS等快速、简便的检测手段扩展。本文对上述两部分内容进行综述,旨在为涉及临床棘白菌素使用及药敏检测工作提供一定的参考信息。
一、念珠菌和曲霉对棘白菌素的敏感性及耐药率变迁
美国微生物学会和欧洲临床微生物与感染性疾病学会均颁布了针对侵袭性念珠菌病诊断及治疗的相关指南,其中针对中重度念珠菌血症患者推荐使用棘白菌素作为一线治疗药物;且大量研究表明这一举措能够显著提升念珠菌血症患者预后[6, 7]。除近平滑念珠菌以及季也蒙念珠菌对棘白菌素类抗真菌药持天然耐药或低敏感状态外,棘白菌素对大多数念珠菌具有杀菌效应[8, 9]。棘白菌素还是治疗多重耐药耳念珠菌的前线药物[10]。随着棘白菌素临床使用程度的增加,获得性棘白菌素耐药念珠菌的临床分离率也在逐渐升高,由其导致的临床治疗失败案例也不断增多,并引起国际广泛关注。2013年SENTRY真菌鉴测项目对收集自全球31个国家的1514株念珠菌临床分离株进行体外抗真菌药物敏感性调研,结果显示:不同念珠菌种对棘白菌素体外耐药率为0-2.8%不等,其中以光滑念珠菌对阿尼芬净体外耐药率最高[11]。美国杜克医院2001-2010十年间光滑念珠菌对棘白菌素的耐药率从4.9%增至12.3%,且80%耐药菌株感染临床治疗失败[12]。我国大规模多中心侵袭性真菌监测网(CHIF-NET)2010-2014年研究数据显示,光滑念珠菌对棘白菌素的耐药率低于1%,另有约2%光滑念珠菌对棘白菌素呈体外中介状态,而白念珠菌、近平滑念珠菌、克柔念珠菌、热带念珠菌等对棘白菌素的敏感性则高于99.5%[13]。CHIF-NET 2015-2017年研究数据显示,除近平滑念珠菌和季也蒙念珠菌外,三种棘白菌素药物对常见的念珠菌种依然保持良好的体外抗菌活性,耐药率或非野生型菌株比例低于4%[14]。
尽管棘白菌素并未用作治疗IA的一线药物,但是对于唑类耐药烟曲霉感染患者,伏立康唑联合卡泊芬净(或两性霉素B)仍可用作替补治疗手段。现有资料表明,临床常见曲霉菌种(包括烟曲霉、黄曲霉、黑曲霉、土曲霉、构巢曲霉、杂色曲霉)对棘白菌素无天然耐药现象,但目前已发现一些曲霉隐蔽种(cryptic species)可对棘白菌素呈低敏感或天然耐药状态,如黄曲霉复合群中的洋葱曲霉种(A. alliaceus)普遍对棘白菌素天然耐药,烟曲霉复合群中的迟缓曲霉种(A. lentulus)部分菌株可对棘白菌素呈天然耐药,且这些曲霉隐蔽种在西方国家已有临床感染病例报道[15, 16]。近些年SENTRY等全球性真菌鉴测项目调研数据显示,棘白菌素对曲霉临床分离株仍然有着良好的体外敏感性[11]。2017年美国Perlin DS等人报道了全球第一例慢性肺曲霉病患者棘白菌素治疗过程中出现烟曲霉米卡芬净耐药,并发现其耐药与靶基因FKS1突变相关[17, 18]。后续有棘白菌素耐药黄曲霉菌株的研究报道,且其耐药机制可能与靶基因FKS1无关,在FKS1热点区域未检测到突变,其耐药可能涉及其他基因参与[19]。现阶段我国尚未发现获得性棘白菌素耐药曲霉菌株。
二、棘白菌素药敏检测方法
现有较成熟的棘白菌素体外敏感检测方法包括微量肉汤稀释法、纸片扩散法和E-test三类;此外,分子水平检测技术如MALDI-TOF MS和棘白菌素耐药基因FKS突变检测手段因其快速、与标准方法一致性好等优点也逐渐崭露头角。
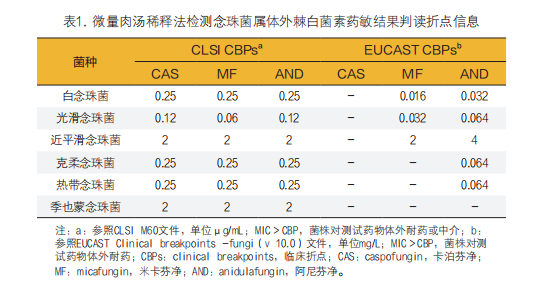
1. 念珠菌棘白菌素药敏试验:美国临床实验室标准化委员会(CLSI)和欧盟药敏试验标准化委员会(EUCAST)均建立了针对酵母菌棘白菌素体外敏感性检测的微量肉汤稀释法药敏方案,即CLSI M27(2017)和EUCAST v9.3.2(2020)文件[20, 21]。但是,鉴于标准微量肉汤稀释法药敏试验操作流程较为繁琐,且在药敏结果终点判读上存在个人差异,特别是针对酵母菌唑类及棘白菌素敏感性测定方面,因其取50%抑制MIC为终点,其判读结果在不同检验人员间存在一定肉眼差异。现阶段这两种标准药敏方案在我国大多数临床微生物实验室未常规开展,主要用于科学研究实验及流行病学监测项目。CLSI M60文件颁布了常见念珠菌对棘白菌素药敏结果判读的临床折点信息(clinical break points,CBPs)[22];EUCAST于2020年颁布了针对部分念珠菌(包括白念珠菌、光滑念珠菌、近平滑念珠菌)的米卡芬净和阿尼芬净药敏CBPs,以及克柔念珠菌和热带念珠菌的米卡芬净药敏CBPs,鉴于卡泊芬净药敏结果在不同实验室间分布差异较大,现未制定其任何折点信息,但建议对于米卡芬净和阿尼芬净持体外敏感状态的念珠菌也应认为其对卡泊芬净体外敏感[23]。
美国赛默飞世尔公司研发的Sensititre YeastOne YO10真菌药敏检测系统可用于检测念珠菌对包括三种棘白菌素在内的9种抗真菌药物的体外敏感性,通过在检测体系中加入亚甲蓝显色剂,根据真菌生长繁殖产生CO2引起检测体系pH值降低,进而使指示剂颜色发生改变,且其变化程度与真菌生长状态具有关联性,辅助读取终点最小抑菌浓度(minimal inhibitory concentration,MIC),一定程度上能够弥补标准微量肉汤稀释法所面临的因检测人员视觉差异带来的结果误差。大量研究证明,Sensititre YeastOne YO10在念珠菌体外棘白菌素敏感性检测方面与标准微量肉汤稀释法结果一致性好,有能力用于临床常规真菌药敏检验工作中[24, 25]。
此外,CLSI还颁布了念珠菌纸片扩散法体外药敏检测方案(CLSI M44文件),该方案可用于检测念珠菌棘白菌素体外敏感性,但在我国其应用程度有限[26]。E-test亦可用于念珠菌体外棘白菌素敏感性检测,且市面上已有商品化棘白菌素E-test检测试条,有研究表明,E-test在检测念珠菌米卡芬净和阿尼芬净体外敏感性上与EUCAST微量肉汤稀释法一致性较好,但在卡泊芬净敏感性检测方面,一致性略差,易将小部分(约8%)受试念珠菌错判为卡泊芬净体外耐药[24]。另有研究人员分别采用Vitek 2,E-test和CLSI微量肉汤稀释法检测100株念珠菌对卡泊芬净和米卡芬净的敏感性,结果显示CLSI与E-test方法的结果间一致性高[27]。
念珠菌FKS基因突变与棘白菌素耐药密切相关,因此可通过检测菌株FKS基因突变型别来推断其对棘白菌素的敏感性[28]。有研究从199株耳念珠菌中检测出10株棘白菌素耐药株,对10株耐药菌株进行FKS1基因检测,并通过动物实验验证这些耐药菌株在模型小鼠体内对棘白菌素治疗的反应性,发现不同FKS1突变基因型在对棘白菌素药物的反应性上存在差异,并提出通过检测FKS1基因型能够较体外药敏试验MIC结果更好地预测体内治疗效果[29]。MALDI-TOF MS在快速检测细菌体外抗生素敏感性方面已有较多研究基础并较强的应用前景,有研究人员尝试通过该方法检测念珠菌体外棘白菌素敏感性,研究表明其检测结果与标准微量肉汤稀释法结果一致性较高(>90%),且该方法可以在6个小时内得到检测结果,显著缩短检测时长,有助于该方法在临床实验室的推广使用[30-32]。
2. 曲霉棘白菌素药敏试验:它与念珠菌属不同的是,棘白菌素对曲霉属仅发挥抑菌作用而无杀菌效果,通过溶解扩展菌丝顶端结构,改变细胞壁组分及菌丝形态,抑制曲霉生长能力。这一特征使得其在体外药敏试验结果判读上与念珠菌存在差别,MIC显然不适用于曲霉棘白菌素敏感性检测,相应地,研究人员提出了最小有效浓度(minimal effective concentration, MEC)这一概念,即相对于生长对照孔,读取使检测孔菌丝体呈现卷曲成团生长的棘白菌素最低浓度,这一概念更符合棘白菌素抗曲霉作用机制,一定程度上能够更好地反映实际药敏情况。E-test是现阶段我国微生物实验室对曲霉等丝状真菌进行唑类及两性霉素B药物敏感性检测的常用方法,但是在曲霉棘白菌素药敏检测方面,因其MEC终点判读较为困难,目前该方法并未在国内微生物实验室得以应用。基于微量肉汤稀释法的抗真菌药物敏感性检测试验是现阶段针对曲霉棘白菌素体外敏感性检测的主要方法亦是标准方法,可评估药物包括卡泊芬净、米卡芬净和阿尼芬净。CLSI和EUCAST分别制定了针对曲霉等产孢丝状真菌体外抗真菌药物敏感性检测方案,即CLSI M38-A3(2017)和EUCAST E.DEF 9.3.2(2020)文件;两种方案针对曲霉棘白菌素敏感性检测均推荐读取MEC[33, 34]。此外,CLSI M59(2020)文件还颁布了针对四种常见曲霉(即烟曲霉、黄曲霉、黑曲霉和土曲霉)的卡泊芬净流行病学临界值(epidemiological cut-off value,ECV),根据该ECV标准可将受试曲霉分为卡泊芬净野生型(wild type,WT)和非野生型(non-wild type,NWT)两类,但两类菌株与棘白菌素实际临床治疗效果间的关联性仍不十分明确;EUCAST尚未制定针对曲霉棘白菌素敏感性检测的临床折点信息。鉴于上述两种标准药敏检测方案在操作上均较繁琐,尚未在临床微生物实验室得以大规模展开,现多用于流行病学监测调研项目。Arendrup MC等学者尝试通过向培养体系中加入颜色指示剂以及制备含有棘白菌素不同药物浓度的培养平板来优化药敏检测流程,筛选棘白菌素耐药曲霉菌株,取得了较好的效果[35, 36]。此外,Sensititre YeastOne YO10抗真菌药敏检测系统也可用于检测曲霉棘白菌素体外敏感性,相关的一致性评估工作开展也较多,总体一致性良好[37, 38]。
3. 棘白菌素“矛盾现象”:多项体外研究表明,棘白菌素类抗真菌药物对念珠菌属和曲霉属均可产生“矛盾现象”(又称“Eagle effect”)[39, 40],即在低药物浓度时对念珠菌或曲霉发挥杀菌或抑菌效应,而在高药物浓度时反而出现菌落生长的现象,在临床药敏检测过程中应予以留意。目前该现象的产生机制及与临床治疗的相关性尚不十分明确。
三、小结
现阶段,棘白菌素仍为治疗侵袭性真菌病的有效抗真菌药物,除小部分棘白菌素天然耐药真菌菌种外,获得性棘白菌素耐药念珠菌的临床分离率有升高趋势,棘白菌素耐药曲霉菌株的分离率仍维持在低水平。但是随着棘白菌素临床使用程度的不断增加,后续棘白菌素耐药菌株的持续动态监测仍可不忽视。对于有条件的微生物实验室,可以采用微量肉汤稀释法或者商品化试剂盒检测受试真菌的棘白菌素药物敏感性;准确快捷的新兴分子手段检测棘白菌素药物敏感性技术日趋成熟,日后有望应用到微生物常规检验工作中。
参考文献
Donnelly JP, Chen SC, Kauffman CA, et al. Revision and update of the consensus definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium [J]. Clin Infect Dis, 2020, 71(6):1 367-1376.
Souza L, Nouér SA, Morales H, et al. Epidemiology of invasive fungal disease in haematologic patients [J]. Mycoses, 2021, 64(3): 252-256.
Stan CD, Tuchiluş C, Stan CI. Echinocandins--new antifungal agents [J]. Rev Med Chir Soc Med Nat Iasi, 2014, 118(2): 528-536.
Lepak AJ, Andes DR. Echinocandins. Encycl Mycol, 2021, 1:438-448.
Pristov KE, Ghannoum MA. Resistance of Candida to azoles and echinocandins worldwide [J]. Clin Microbiol Infect, 2019, 25(7): 792-798.
Ullmann AJ, Cornely OA, Donnelly JP, et al. ESCMID guideline for the diagnosis and management of Candida diseases 2012: developing European guidelines in clinical microbiology and infectious diseases. Clin Microbiol Infect, 2012, 18 Suppl 7: 1-8.
Pappas PG, Kauffman CA, Andes DR, et al. Executive summary: clinical practice guideline for the management of candidiasis: 2016 update by the infectious diseases society of America [J]. Clin Infect Dis, 2016, 62(4): 409-417.
Banche G, Mandras N, Giacchino F, et al. Caspofungin benefit on phagocytes from patients with renal dysfunction infected with multidrug-resistant Candida glabrata [J]. Future Microbiol, 2013, 8(9): 1091-1096.
Perlin DS. Echinocandin resistance in Candida [J]. Clin Infect Dis, 2015, 61(Suppl 6): S612-7.
Sears D, Schwartz BS. Candida auris: an emerging multidrug-resistant pathogen [J]. Int J Infect Dis, 2017, 63: 95-98.
Castanheira M, Messer SA, Rhomberg PR, et al. Antifungal susceptibility patterns of a global collection of fungal isolates: results of the SENTRY antifungal surveillance program (2013) [J]. Diagn Microbiol Infect Dis, 2016, 85(2): 200-204.
Alexander BD, Johnson MD, Pfeiffer CD, et al. Increasing echinocandin resistance in Candida glabrata: clinical failure correlates with presence of FKS mutations and elevated minimum inhibitory concentrations [J]. Clin Infect Dis, 2013, 56(12): 1724-1732.
Xiao M, Fan X, Chen SC, et al. Antifungal susceptibilities of Candida glabrata species complex, Candida krusei, Candida parapsilosis species complex and Candida tropicalis causing invasive candidiasis in China: 3 year national surveillance. J Antimicrob Chemother, 2015, 70(3): 802-810.
Xiao M, Chen SC, Kong F, et al. Distribution and Antifungal Susceptibility of Candida Species Causing Candidemia in China: An Update From the CHIF-NET Study [J]. J Infect Dis, 2020, 221(Suppl 2): S139-S147.
Alastruey-Izquierdo A, et al. Antifungal susceptibility profile of cryptic species of Aspergillus [J]. Mycopathologia, 2014, 178(5-6): 427-433.
Tsang CC, Tang JYM, Ye H, et al. Rare/cryptic Aspergillus species infections and importance of antifungal susceptibility testing [J]. Mycoses, 2020, 63(12): 1283-1298.
Jiménez-Ortigosa C, Moore C, Denning DW, et al. Emergence of echinocandin resistance due to a point mutation in the fks1 gene of Aspergillus fumigatus in a patient with chronic pulmonary aspergillosis [J]. Antimicrob Agents Chemother, 2017, 61: e01277-17.
Satish S, Jiménez-Ortigosa C, Zhao Y, et al. Stress-induced changes in the lipid microenvironment of β-(1,3)-d-glucan synthase cause clinically important echinocandin resistance in Aspergillus fumigatus [J]. mBio, 2019, 10(3): e00779-19.
Yassin Z, Lotfali E, Khourgami MR, et al. Caspofungin resistance in clinical Aspergillus flavus isolates [J]. J Mycol Med, 2021, 31(4): 101166.
CLSI. 2020. Reference method for broth dilution antifungal susceptibility testing of yeasts. CLSI document M27. Clinical and Laboratory Standards Institute, Wayne, PA.
EUCAST. 2020. Method for the determination of broth dilution minimum inhibitory concentrations of antifungal agents for yeasts. E.DEF 7.3.2. European Committee for Antimicrobial Susceptibility Testing.
CLSI. Performance standards for antifungal susceptibility testing of yeasts, 2nd Edition. CLSI document M60. Clinical and Laboratory Standards Institute, Wayne, PA.
EUCAST. Antifungal agents breakpoint tables for interpretation of MICs, version 10.1. European Committee for Antimicrobial Susceptibility Testing.
Aigner M, Erbeznik T, Gschwentner M, et al. Etest and Sensititre YeastOne susceptibility testing of ehinocandins against Candida species from a single center in Austria [J]. Antimicrob Agents Chemother, 2017, 61(8). pii: e00512-17.
Espinel-Ingroff A, Alvarez-Fernandez M, Cantón E, et al. Multicenter study of epidemiological cutoff values and detection of resistance in Candida spp. to anidulafungin, caspofungin, and micafungin using the Sensititre YeastOne colorimetric method [J]. Antimicrob Agents Chemother, 2015, 59(11): 6725-6732.
CLSI. Method for Antifungal disk diffusion susceptibility testing of Yeasts, 2nd Edition. CLSI document M44. Clinical and Laboratory Standards Institute, Wayne, PA.
Upadhyay S, Sarma S, Chowdhary A. Comparative analysis of antifungal susceptibility testing methods for echinocandins in candidemia isolates [J]. International Journal of Infectious Diseases, 2020, 101(Suppl 1): 388.
Zhao Y, Nagasaki Y, Kordalewska M, et al. Rapid detection of FKS-associated echinocandin resistance in Candida glabrata [J]. Antimicrob Agents Chemother, 2016, 60(11): 6573-6577.
Sharma D, Paul RA, Rudramurthy SM, et al. Impact of FKS 1 genotype on echinocandin in-vitro susceptibility in Candida auris and in-vivo response in a murine model of infection [J]. Antimicrob Agents Chemother, 2022, 66(1): e0165221.
Vella A, De Carolis E, Mello, et al. Potential use of MALDI-TOF mass spectrometry for rapid detection of antifungal resistance in the human pathogen Candida glabrata [J]. Sci Rep, 2017, 7(1): 9099.
Vatanshenassan M, Boekhout T, Meis JF, et al. Candida auris identification and rapid antifungal susceptibility testing against echinocandins by MALDI-TOF MS [J]. Front Cell Infect Microbiol, 2019, 9:20.
Vatanshenassan M, Arastehfar A, Boekhout T, et al. Anidulafungin susceptibility testing of Candida glabrata isolates from blood cultures by the MALDI Biotyper antibiotic (antifungal) susceptibility test rapid assay [J]. Antimicrob Agents Chemother, 2019, 63(9): e00554-19.
CLSI. 2017. Reference method for broth dilution antifungal susceptibility testing of filamentous fungi. CLSI document M38. Clinical and Laboratory Standards Institute, Wayne, PA.
EUCAST. 2020. Method for the determination of broth dilution minimum inhibitory concentrations of antifungal agents for conidia forming moulds. E.DEF 9.3.2. European Committee for Antimicrobial Susceptibility Testing.
Meletiadis J, Siopi M, Kanioura L, et al. A multicentre study to optimize echinocandin susceptibility testing of Aspergillus species with the EUCAST methodology and a broth microdilution colorimetric method [J]. J Antimicrob Chemother, 2020, 75(7): 1799-1806.
Meletiadis J, Siopi M, Kanioura L, et al. Development and multicentre validation of an agar-based screening method for echinocandin susceptibility testing of Aspergillus species [J]. J Antimicrob Chemother, 2019, 74(8): 2247-2254.
Siopi M, Pournaras S, Meletiadis J. Comparative evaluation of Sensititre YeastOne and CLSI M38-A2 reference method for antifungal susceptibility testing of Aspergillus spp. against echinocandins [J]. J Clin Microbiol, 2017, 55(6): 1714-1719.
Lyskova P, Hubka V, Svobodova L, et al. Antifungal susceptibility of the Aspergillus viridinutans complex: comparison of two in vitro methods [J]. Antimicrob Agents Chemother, 2018, 62(4): e01927-17.
张明, 施毅. 棘白菌素类抗真菌药物的“矛盾现象”[J]. 中国感染与化疗杂志, 2014, 14(5): 442-445.
Steinbach WJ, et al. Potential microbiological effects of higher dosing of echinocandins [J]. Clinical Infectious Diseases, 2015, 61(S6): S669-677.
作者单位:100053北京,首都医科大学宣武医院检验科
通讯作者:王培昌


